By Arthur Geary 
Once you identify the practice goals you want to achieve and have put the right leadership and culture in place, it is up to you as practice CEO to tie all of these elements together to execute your plans.
There are five key ingredients that you, as practice leader, need to bring together to make your business plans a reality: people, strategic plans, tactics, process/implementation and benchmarks. Each of these elements is not only necessary in and of itself, but also to support the other elements. For example, without the right staff in place, you will not be able to implement your plans, and without the right benchm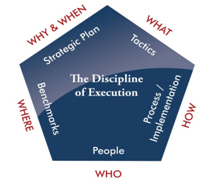 arks, you will never to be able to gauge whether you have achieved your goals.
arks, you will never to be able to gauge whether you have achieved your goals.
Here is a summary of these five key ingredients and how they work together.
Strategic Plan: This can be a new initiative, program, project, or other type of specific goal; perhaps a goal generated from an important benchmark variance. As practice leader, you need to state the goal as specifically as possible and answer the questions: Why are we doing this? When is completion expected? Some examples of practice goals are:
–Increase patient volume from 800 exams/month to 1,200 exams/months by December 31, 2011 to offset declining third-party reimbursements.
–Improve Quality Service Survey scores of “Excellent” from 88 percent to 95 percent by Oct. 31, 2011 to improve existing patient exams.
–Open two new full-time offices by June 30, 2012 to grow the practice by 50 percent in calendar year 2013.
–Integrate the meaningful use of an EHR system by December 31, 2011 to qualify for the federal reimbursement.
–Reduce staff turnover from 42 percent to 15 percent by the end of calendar year 2011 to improve quality of patient care and doctor satisfaction.
–Implement rational staff compensation and reduce as a percentage of revenue from 24 percent to 20 percent for fiscal year 2012 to improve net profit and reduce staff complaints of fairness.
Years ago, as president of a large multi-location regional optometric practice with 150 employees, I set as a goal to dramatically improve our customer service impact on patients, while also improving the friends and family atmosphere of our staff and offices. As part of this upgrade we set as a tactic that all front desk personnel and technicians were to greet patients by introducing themselves and shaking the patient’s hand. In addition, the front desk people, because they are seated behind the front counter, were to stand, smile and make eye contact with each patient as they welcomed them to the practice.
I discussed the plan with my executive staff, all of our office managers, and representatives from our front desk and technical staff.
The consensus from my executive staff and office managers was that this was a good idea and would have a big impact on WOWing our patients. However, our front desk staff and technicians had a completely different view. You would have thought I asked them to kiss every patient on the lips or to do jumping jacks every time a patient walked in! Needless to say, we uncovered many unexpected objections and ultimately had to modify the policy by dropping the hand shake. In the end, the revised policy had a huge positive impact on patients, and staff eventually took pride in the level of customer service we provided that was well above any other competitor.
People: Every organization is only as good as its people. I realize many consider that an overused cliché, but I believe it’s as true today as ever. Any plan, initiative, program, project or goal is dependent on WHO is involved. Therefore, this is typically the next element I like to integrate because it impacts all the other elements: who interacts with the patients; who is responsible for how the plan is implemented; who will employ what tactics to support attainment of the goal; who will do the measuring or benchmarking and report on where results are in relation to the goal?
The process for identifying the people you need to achieve your goals is not linear in that you might start with the strategy and shift to an assessment of the people necessary to handle the additional volume; then shift to an assessment of the implementation plan and additional training or hiring necessary; then back to the strategic plan to account for the additional time anticipated for hiring and training, etc.
Let’s use the first example from above to illustrate our point: Increase patient volume from 800 exams/month to 1,200. That’s a 50 percent increase!
The people issues become: can the existing doctor staff handle it? If not, how many more are needed? What is the recruiting time frame? Is additional staff necessary? If so, how long will it take to recruit and train them? Can our internal lab accommodate 50 percent more jobs? Will marketing staff be needed for community outreach programs as part of the growth strategy?
Tactics/Resources: What are you going to do to support, promote or advance the attainment of the goal, whatever it may be? This will vary based on the plan, initiative, program or goal. It may be external as in advertising, community events or promotions. It may be internal as in merchandising, marketing, signage, contests or employee communications and incentives. For this element the key considerations will typically be lead time, program design, margins, budgets and any other necessary resources. Success in this element not only depends on adequate human resources, but the crafting of the appropriate message, visual concept, program, media and planning for fulfillment on the back end, whether that be through staff or another delivery method, which ultimately ties it back to process and implementation. The related resources may include money, expertise, staff or other unique practice-specific resources.
Process/Implementation: How will all the plans, goals, tactics, associated process modifications, training and hiring be planned and coordinated to achieve the desired results? This element of execution integrates heavily with the people element to drive behavior through the organization and down to the most important component–patient interaction. Integrating the plan, the people, and the operational processes and implementation are the most critical elements of execution. Inadequate focus on this element is the most common cause of what is perceived to be a dysfunctional organization. This is often caused because inadequate time and resources are committed to communicating the plan and the training material, along with the expected behaviors and incentives. Too often, especially in smaller businesses, time is an issue and much of the communication is done verbally.
Unfortunately, people remember a fraction of what is communicated verbally, and without a written document to refer back to, there is often confusion that leads to errors. Poor training results in poor patient interactions and is compounded by frustrated employees. Fumbling on this element can result in an organization that is resistant to change because they don’t trust management’s ability to execute, and they associate new plans, programs, initiatives and goals with PAIN.
In this case, let’s use the example of incorporating new technology, whether it is diagnostic, optical or practice management-related. There are going to be many assumptions regarding staffing requirements, necessary training, flow, billing and patient satisfaction. It is imperative to get people from each area involved early to test the assumptions. Expect modifications.
Benchmarks/Milestones: This is one of the most important business tools available. You cannot effectively manage a practice if you don’t know where you have been, where you want to go, and where you currently are in relation to where you want to be. However, benchmarking has two important roles to play as an element of execution.
First, benchmarking plays a central role in grounding the organization and all efforts of execution. It may also initiate the execution process as variances from established industry standards up or down may dictate corrective actions or updated plans. As an element of the execution process, at the outset benchmarks may help establish goals, or test proposed goals and assumptions against reality. During the implementation phase benchmarking will keep management grounded in reality so that appropriate adjustments can be made if necessary.
Using the first example again, some useful benchmarks might be:
• Year-over-year exam volume
• Average revenue per doctor hour worked
• Average revenue per exam
• Average time from check-in to check-out
• Average optical revenue per optical sale
There are others that can be tracked, but these will alert you to whether or not you are generating the anticipated additional volume, and whether you have the staffing model right. If your average revenue figures are falling, and the average time in the office is rising, it is likely that you are under-staffed and patient satisfaction is falling.
Second, and equally important, benchmarking is critical for behavior modification, or molding behavior to beliefs to get desired results. To maximize execution you must take the time to align incentives and consequences with the achievement of stated goals as measured by the benchmarks, or consequences for the failure to do so. These then need to be tied back to the people and the implementation process. Clearly communicating goals, incentives and consequences, and consistently holding staff accountable to them, drives behavior. Consistently getting the desired behavior gets the desired results.
An old adage in business is that you can’t manage what you can’t measure/track. Above are a few examples of readily available measures with today’s practice management systems. Other examples are patient surveys and secret shoppers.
Execution is a disciplined process that leads to faster growth and higher profitability and bridges the gap between goals/expectations and results. Practices that embrace this discipline are thoughtful about their focus and what new initiatives they pursue. They don’t waste resources, time, money and energy on ill-conceived or poorly planned initiatives. This results in higher profitability. Whatever these businesses pursue, their people and the implementation plan are integrated with the goal, and milestones are linked to incentives that drive the desired behaviors. As a result, staff morale is higher and turnover is lower. Most importantly, patients encounter behaviors that foster an excellent experience in your practice and patient loyalty because their expectations were met or exceeded. This results in faster growth!
Related ROB Articles
Close the Execution Gap: Top 4 Roadblocks to Execution of Business Plans
Bridge the Execution Gap: Evaluate Yourself as Practice CEO
Establish a Culture of Execution to Achieve Practice Goals
This is the third in a series of articles examining the discipline of execution in business: Bridge the Execution Gap: Leadership-Culture-Process, the 3 Pillars that Support Execution, and Will Take Your Practice From Business Plan to RESULTS!
Arthur Geary, founder and CEO of Execution in Business, Inc., is a senior executive and leader with a broad range of experience from start-up to Fortune 500 companies in eyecare, insurance, finance and securities, medical software and commercial construction. To contact him: ageary@executioninbusiness.com.




















