By Aaron Neufeld, OD
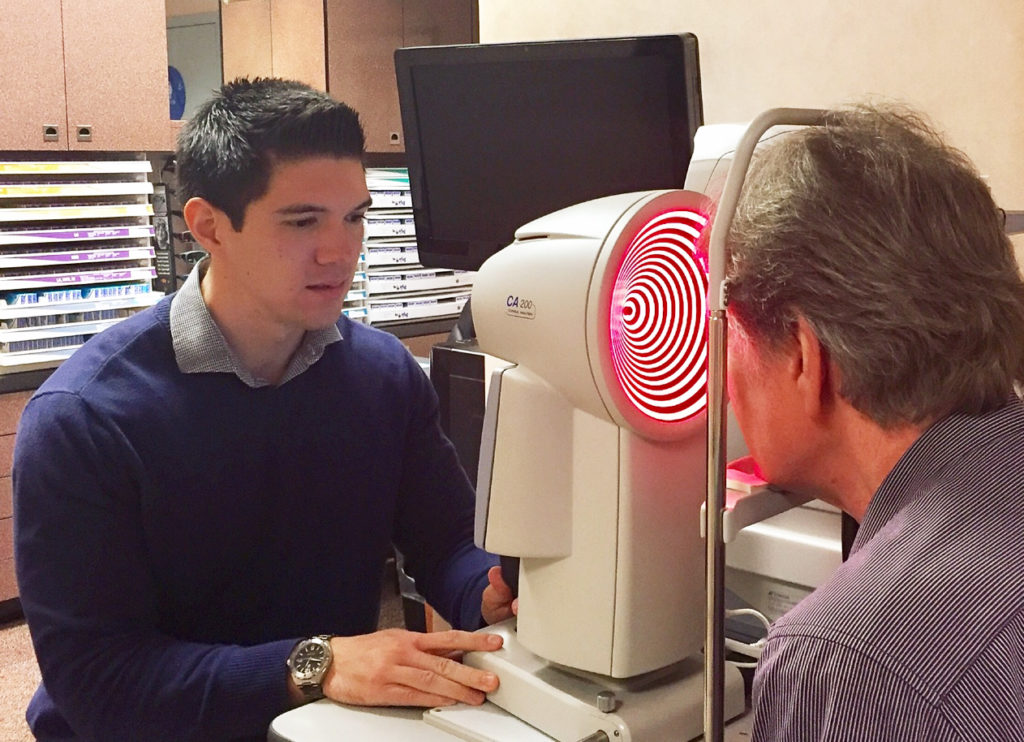
Dr. Neufeld performing corneal topography on a patient. Dr. Neufeld says the corneal topographer is a key instrument to serve Ortho-K patients. The technology also can be used with other patients, making it easier to break even, and profit from.
Jan. 18, 2017
Myopia control with contact lenses and other treatments, like Ortho-K, is a practice growth opportunity and practice differentiator.
Myopia control is a clinical practice in which an eyecare practitioner attempts to circumvent the presumed progression of myopia in a patient (child or adolescent). Myopia progression is thought to occur because of factors such as genetics and time spent doing near work versus outdoor activities.
Over the last 10 years, the myopia control sector of my practice has grown to account for about 5 percent of practice revenue. With the increased prevalence of myopia due to extensive near and computer work in children (especially in our region – the San Francisco Bay Area), I expect this revenue to at least double in the next few years. A myopia control patient generates additional revenue, patient referrals, and an exciting “specialty” niche if done correctly.
The demographics of my practice in Los Altos, Calif., are amenable to a myopia control niche. Myopia has been shown to be more prevalent among Asian-Americans than other ethnic groups, so with 25 percent of my patients Asian-Americans, offering this service is a good fit for us. But more importantly, we are in a very affluent area, so there is a lot of disposable income. Myopia control has become a big priority for many upper-income Asian-American families. (The CRT lenses we use (Paragon) actually send us brochures specifically geared toward a) Asian-Americans and b) the rest of the population!)
In addition, we pull patients from surrounding cities that have higher population densities of Asian-Americans than Los Altos.
Traditional school of thought present five different methodologies in achieving myopia control:
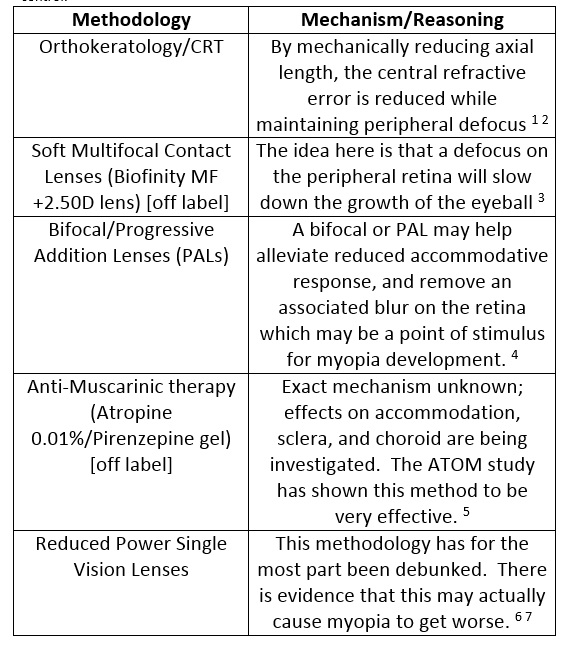
In our practice, we focus mostly on orthokeratology/CRT to control myopia. To a smaller patient population, we also offer soft multifocal contact lenses and bifocals/PALs as alternative myopia control treatments, if a patient and his or her parents do not wish to pursue CRT.
We avoid prescribing reduced power single-vision glasses due to lack of proven efficacy. We also avoid anti-muscarinic therapy due to associated side effects and patient aversion to off-label use (this is a viable option that many other practitioners use, however).
Create Additional Revenue Streams
It is tough to address revenue generation potential in a direct sense, since we incorporate myopia control into other services, such as contact lenses. But looking at our CRT patient base, we have about 40 patients that are in CRTs primarily due to parent concern over myopia progression. This population results in about $50,000-$60,000 in revenues annually from fittings and materials. PALs and soft multifocal contact lenses also bring in additional revenue since materials are priced higher than single-vision alternatives.
Besides adding revenue, implementing myopia control also serves as a practice builder. As a practitioner who is well versed in myopia control, and offering relevant services, you can influence patient perception. You enable yourself to further differentiate as an authority in your field. It sets you apart from your competition. It can also serve as an additional tool for referral.
Revenue comes from both services and materials. When I say “services,” there is not necessarily a visit specifically for myopia control. Services instead encompass comprehensive exams and contact lens fittings.
Myopia control is primarily promoted through our Ortho-K/CRT campaign. We have sections on our web site under Ortho-K/CRT that describe myopia control. It is also alluded to in our CRT ads.
Our largest revenue producer related to myopia control is definitely CRT. A large majority of our CRT fits happen because a patient’s parent becomes concerned about myopia progression in his/her child. I educate the parent on the potential benefits in myopia control that CRT lenses can have. I also give them information and allow them to do further research if needed.
 How Much Doctor Time Is Required?
How Much Doctor Time Is Required?
This is all dependent on the myopia control method you prescribe to your patient. If you are going the PAL or soft multifocal contact lens route, a regular comprehensive exam followed by one or two follow-up visits is probably all that is necessary. However, if you are fitting a child in CRT lenses, expect a long initial visit for fitting/training, as well as at least four follow-up visits to ensure an accurate fit and good compliance. (Your CRT fit cost should reflect this heavy chair time, logically).
Which Patients Are Good Candidates?
Myopia control services can be used for children and adolescents.
Good candidates for myopia control are patients that fall under one or more of the following three categories:
Myopia creep. Increasing myopia at each annual eye examination. This is subjective and requires a decision from the practitioner. Some regard a –0.50D jump as large, while others may be more liberal and consider a –1.00D jump to be large.
Less Time Outside. Less time outside and more time doing near work may contribute to increasing myopia.
Genetics. Genetic predisposition to myopia: one or both parents are myopic.
What Instruments are Necessary?
Success in fitting CRT lenses requires a corneal topographer. Fortunately, a topographer also can be used for fitting specialty contact lenses. I purchased a corneal topographer outright for $21,000. I broke even indirectly after three years due to the amount of specialty contact lens fits that I have used the topographer for.
Educate Yourself & Staff
Most ODs have general knowledge of myopia progression and myopia control methods that can be utilized. A plethora of peer reviewed articles and scientific data exist on the web, and can be found through a simple Google search.
The Brien Holden Vision Institute releases informative and current research on myopia control. Other optometric publications, such as Review of Optometry, release great informative articles on myopia control periodically.
Support staff who have general knowledge in myopia control can have a positive impact in growing myopia control in your practice. For my practice, all of our staff members are educated on the general causes of myopia and the intervention treatments we offer. Although we do not have our staff preach myopia control, they are able to field questions on the topics and can steer candidates and interested parties toward the doctors, who then provide additional information.
Educate Patients & Parents
We mostly market myopia control through word of mouth and patient education.
The great thing with myopia control, is that more often than not, it is the parent of the patient who brings up the subject. When you have a child sitting in your chair who is about to get their first pair of glasses, or needs to update their glasses or contact lenses due to a prescription increase, inevitably the parent starts to launch questions at you: Why is this occurring? Is it because he plays too many video games? Is this my fault? Bad genes? The list of questions can go on and on. This is the perfect time to step in.
Educate the parent on:
Cause. Why myopia progression occurs – genetics and time spent doing near work vs. outdoor activities.
Complications. Potential pathologies that can result from high myopia (ex: retinal detachment).
Lifestyle enhancement. Quality of life issues that can result from a highly myopic prescription. Next, present options that can potentially reduce myopia. Whether it be CRT, soft multifocal contact lenses, atropine, etc. Try to only present the option which you view as the best fit for the patient. Only mention alternatives at the patient’s request. Remember to speak slowly, use layman terms, and pause frequently for questions. This is uncharted territory for the majority of patients. No parent would ever want their child’s eyesight to continually get worse, so your advice will fall on wishful and often willing ears.
Special Thanks to Dr. Myhanh Nguyen at Coopervision for her help in writing this article.
References
1) “Myopia Prevention and Control.” Contact Lens References Related to Myopia Prevention. N.p., 2012. Web. 17 Jan. 2016
2) Reim TR, Lund M, Wu R. Orthokeratology and adolescent myopia control. Contact Lens Spectrum, 2003. 18(3):40-2.
3) Anstice NS, Phillips JR. Effect of dual-focus soft contact lens wear on axial myopia progression in children. Ophthalmology. 2011 Jun;118(6):1152-61.
4) Gwiazda J, Thorn F, Bauer J, Held R. Myopic children show insufficient accommodative response to blur. Invest Ophthalmol Vis Sci. 1993 Mar;34(3):690-4.
5) Chua WH, Balakrishnan V, Tan D, Chan YH. (2003) Efficacy results from the Atropine in the Treatment Of Myopia (ATOM) study. Invest Ophthalmol Vis Sci 2003;44; ARVO E-Abstract 3119.
6) Myrowitz, Elliott H. “Juvenile Myopia Progression, Risk Factors and Interventions.” Saudi Journal of Ophthalmology. Elsevier, 13 Aug. 2015. Web.
7) Kading, David and Mayberry, Amber. “Slowing Myopia Progression in Children” Review of Optometry. 19 Nov. 2012. Web.
 Aaron Neufeld, OD, is the owner of Los Altos Optometric Group in Los Altos, Calif. To contact: aneufeldod@gmail.com
Aaron Neufeld, OD, is the owner of Los Altos Optometric Group in Los Altos, Calif. To contact: aneufeldod@gmail.com




















